
What Parkinson’s Disease Really Does to Your Body
Imagine your brain sending a signal to move your hand - but the message gets stuck halfway. That’s what happens in Parkinson’s disease. It’s not just shaking. It’s your muscles locking up, your movements slowing down, and your body feeling heavier than it should. At the core, Parkinson’s is about one thing: dopamine - the chemical your brain needs to control smooth, coordinated movement. When dopamine-producing neurons die off, your body loses its ability to move naturally.
By the time most people notice symptoms, they’ve already lost 60 to 80% of these cells. The damage starts quietly, often in just one hand. A slight tremor when resting - like your thumb and finger rubbing together, as if rolling a pill. It’s called a "pill-rolling tremor," and it’s one of the clearest early signs. But not everyone shakes. Some people just feel stiff, slow, or unbalanced. That’s because Parkinson’s doesn’t just affect movement. It disrupts the whole system that tells your muscles when and how to move.
The Three Big Symptoms: Tremor, Stiffness, and Slowness
Tremor is what most people think of first. About 80% of people with Parkinson’s experience it, but it doesn’t happen all the time. It shows up when you’re relaxed - sitting, watching TV, or waiting in line. The moment you reach for your coffee cup, it disappears. It’s gone during sleep, too. Stress, fatigue, or strong emotions can make it worse. But tremor alone doesn’t mean you have Parkinson’s. Many older adults have harmless tremors. What sets Parkinson’s apart is the combination.
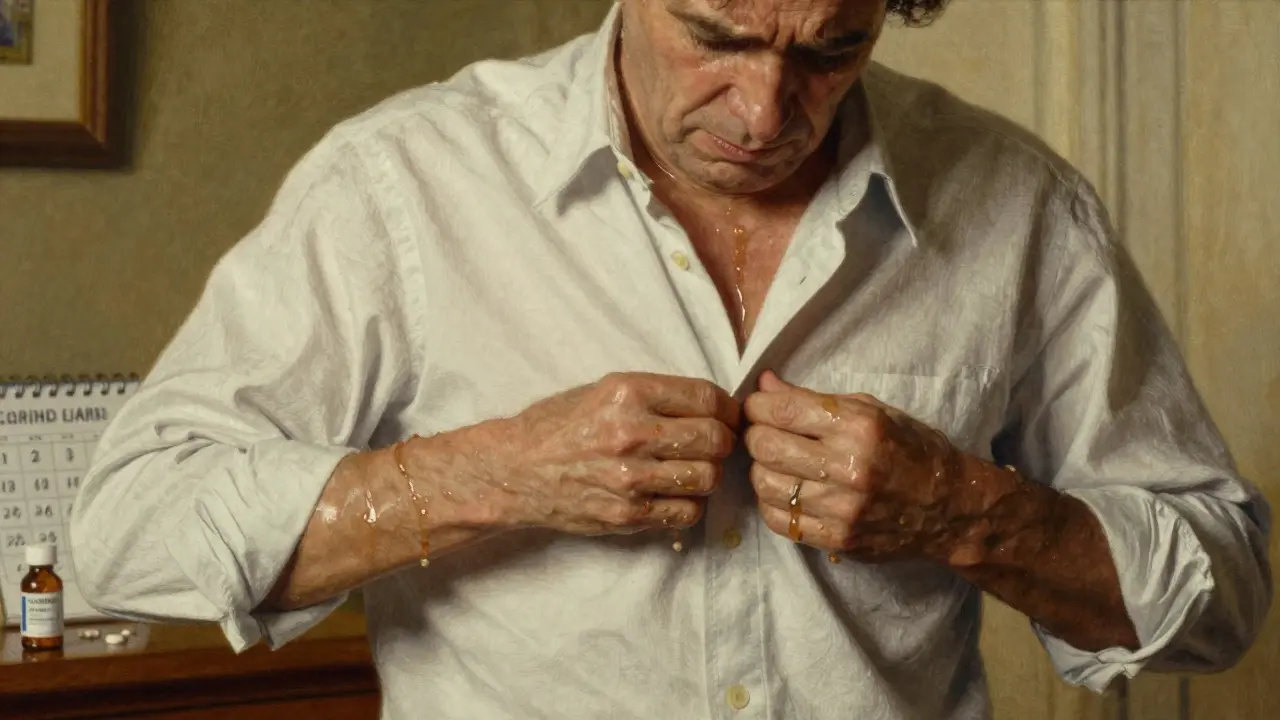
Stiffness - or rigidity - is just as common. It’s not just tight muscles. It’s your arms or legs feeling stuck, like they’re moving through thick syrup. Doctors call it "cogwheel" rigidity when they feel a jerky resistance while moving your limb, or "lead-pipe" when it’s smooth but constant. This stiffness makes everyday things hard: buttoning a shirt, writing your name, tying your shoes. A study from Parkinson’s UK found that 73% of people struggle with these tasks within three years of diagnosis.
Then there’s bradykinesia - the medical term for slowness of movement. It’s not laziness. It’s your brain taking longer to send the signal to move. Getting up from a chair feels like a chore. Walking becomes small, shuffling steps. Your face loses expression. Your voice softens. These changes creep in slowly. Many people don’t realize it’s Parkinson’s until someone else points it out.
Why Dopamine Replacement Is the Main Treatment
Your brain makes dopamine naturally. In Parkinson’s, it stops. So doctors replace it - not by giving dopamine itself, but by giving levodopa, a chemical your brain can turn into dopamine. Levodopa crosses the blood-brain barrier. Other drugs can’t. That’s why it’s the gold standard.
But levodopa alone causes side effects like nausea and dizziness because your body converts it to dopamine too early - in your stomach and blood, not your brain. That’s why it’s almost always paired with carbidopa. Carbidopa blocks that early conversion, letting more levodopa reach your brain. Together, they form the most common treatment: carbidopa/levodopa. It’s been used since the 1970s, and it still works better than anything else.
For most people, the results are dramatic. Within 30 to 60 minutes of taking a dose, stiffness eases, tremors quiet down, and movement becomes easier. Studies show up to 70% improvement in motor symptoms during the first few years. This is called the "honeymoon period." For many, it’s life-changing. You can walk again. You can write. You can get dressed without help.
What Happens When the Medication Stops Working
The problem isn’t that levodopa stops working. It’s that your brain changes over time. After 5 to 10 years, the effects don’t last as long. You start noticing "wearing-off" - your good hours shrink. You take your pill at 8 a.m., feel great until noon, then suddenly, you’re stiff again. That’s not your disease getting worse - it’s your body’s ability to store and use dopamine fading.
Then come the unpredictable "on-off" swings. One minute you’re moving fine. The next, you’re frozen. It feels random. And then there’s dyskinesia - involuntary movements. Your leg kicks out. Your head nods. Your arm waves. It’s not your fault. It’s the side effect of too much dopamine in the wrong places. About 40 to 50% of people on long-term levodopa develop this. For some, it’s worse than the original symptoms.
That’s why doctors now start with lower doses. The old advice was to push the dose higher as fast as possible. Now, we know that’s a recipe for early dyskinesia. The "start low, go slow" approach is standard. Most begin with 25/100 mg one to three times a day, slowly increasing based on response.
Alternatives to Levodopa: Dopamine Agonists and More
Not everyone can tolerate levodopa. Some are younger, diagnosed before 50, and doctors want to delay motor complications. That’s where dopamine agonists come in - drugs like pramipexole and ropinirole. They don’t become dopamine. They mimic it by directly stimulating dopamine receptors.
They’re less powerful than levodopa - about 30 to 50% as effective for movement - but they have a lower risk of early dyskinesia. Many people start with one of these, especially if they’re under 60. But they come with their own side effects: dizziness, sleepiness, swelling in the legs, and sometimes impulse control issues - gambling, overeating, compulsive shopping. These aren’t common, but they’re serious.
Many people end up on both. Levodopa for strong symptom control. Agonists to smooth out the edges. About 60% of patients eventually need this combo. It’s not perfect, but it’s the best we have right now.

Practical Tips for Taking Medication Right
Taking your pills correctly is just as important as choosing them. Levodopa competes with protein for absorption in your gut. High-protein meals - eggs, meat, cheese - can block it. That’s why many people are told to take their medication 30 minutes before or an hour after eating. Some even switch to low-protein diets for breakfast and lunch.
Timing matters too. If you’re having "wearing-off" episodes, your doctor might suggest more frequent doses or switching to an extended-release version like Rytary. But Rytary costs about $5,800 a year. The generic version? Around $600. Cost isn’t just a concern - it affects whether you can stick to your plan.
Managing medication becomes a full-time job. On average, people spend 15 minutes a day on it early on. By the moderate stage, it’s 45 minutes. Over 78% of patients need help from a caregiver to keep track. Missed doses, wrong timing, food interference - all of it adds up.
What’s Next? New Treatments on the Horizon
There’s hope beyond pills. In 2018, the FDA approved Inbrija - a powder you inhale during an "off" episode. It works in under 10 minutes. No swallowing. No waiting. But it’s expensive - $3,700 a month. Not everyone can afford it.
Even more promising are continuous delivery systems. In a 2022 trial, a subcutaneous infusion of foslevodopa/foscarbidopa gave patients 2.5 more "on" hours each day compared to oral pills. That’s huge. Imagine not having to plan your day around your next dose.
Gene therapies are still experimental, but they aim to help your brain make its own dopamine again. And researchers are using genetic testing to predict who will respond best to which drug. Variants in the COMT and MAO-B genes may one day guide personalized treatment.
But for now, dopamine replacement - with all its ups and downs - remains the cornerstone. It doesn’t stop the disease. But it gives people back their days.
Living With Parkinson’s: It’s Not Just About Medication
Medication helps you move. But exercise helps you stay strong. Physical therapy keeps your balance. Speech therapy keeps your voice clear. These aren’t extras. They’re essential. Studies show that regular aerobic exercise slows decline more than any drug.
And mental health? It’s often ignored. Depression and anxiety are common in Parkinson’s - not just because of the diagnosis, but because your brain’s chemistry is changing. Talking to someone who gets it - a support group, a counselor - makes a real difference.
Parkinson’s isn’t a death sentence. It’s a long journey. Some people live for decades with good quality of life. Others face tougher challenges. But knowing how the treatment works - and what to expect - helps you take back control.
Is tremor always the first sign of Parkinson’s disease?
No. While tremor is the most recognizable symptom, about 20% of people with Parkinson’s don’t have it at all. Others may notice stiffness, slowness, or trouble with balance first. Some people realize they’re dragging their foot or their handwriting has gotten smaller. Not everyone shakes - and that doesn’t mean it’s not Parkinson’s.
Can dopamine replacement cure Parkinson’s disease?
No. Dopamine replacement - like levodopa - only treats the symptoms. It doesn’t stop the brain cells from dying. That’s why symptoms return and worsen over time. There is currently no cure. But for many, medication allows them to live well for years.
Why does levodopa stop working after a few years?
It doesn’t stop working - your brain changes. As more dopamine-producing cells die, your brain loses its ability to store and release dopamine smoothly. The medication still helps, but the effects don’t last as long. You may need more frequent doses or different formulations. This is called motor fluctuation, and it’s a normal part of disease progression, not a treatment failure.
Can I take levodopa with food?
It’s best to take levodopa on an empty stomach or at least 30 minutes before a meal. High-protein foods like meat, eggs, cheese, and beans compete with levodopa for absorption in the gut. If you take it with a protein-heavy meal, it may not work as well. Many people find success by saving protein for dinner and eating lighter meals earlier in the day.
Are dopamine agonists safer than levodopa?
They have a lower risk of causing dyskinesia (involuntary movements), which is why they’re often used early, especially in younger patients. But they come with other risks - dizziness, sleepiness, swelling, and sometimes compulsive behaviors like gambling or overeating. Levodopa is more effective for movement, but agonists can be a good starting point or add-on. The choice depends on your age, symptoms, and lifestyle.
How do I know if my medication schedule needs adjusting?
If you notice your "on" time shrinking - you’re moving well for only 2 or 3 hours after a dose instead of 4 or 5 - or if you’re experiencing sudden freezing or uncontrolled movements, it’s time to talk to your neurologist. Keep a daily log: note when you take your pills, when you feel good, when you feel stiff or shaky. This helps your doctor fine-tune your plan. Don’t wait until it’s overwhelming.
Managing Parkinson’s isn’t about finding a magic pill. It’s about understanding how your body responds, adjusting over time, and using every tool available - medicine, movement, and support. The goal isn’t perfection. It’s more good days than bad ones.


srishti Jain
This is why I stopped trusting doctors. They act like levodopa is a cure when it's just a band-aid on a bullet wound.
kelly tracy
You call that a "honeymoon period"? That's just the calm before the storm. The moment you get used to moving again, your body starts betraying you in new ways. Dyskinesia isn't a side effect - it's the price of admission.
Nadia Spira
The entire paradigm is flawed. We're treating symptoms like a broken circuit when the real issue is mitochondrial decay and neuroinflammation. Dopamine replacement is 1970s medicine clinging to a 21st-century problem. We need epigenetic reprogramming, not chemical crutches.
Shae Chapman
I just want to say thank you for writing this. My mom has been on levodopa for 8 years and I finally understand why she cries after dinner. 🥺 It’s not sadness - it’s the exhaustion of fighting her own body. This helped me be a better caregiver.
henry mateo
i read this whole thing and just wanted to say… the part about protein interfering with levodopa? my dad just started doing that low-protein breakfast thing and he’s been walking like he’s 40 again. i didnt even know that was a thing. thanks for sharing
Glendon Cone
Honestly, the most powerful thing here isn’t the meds - it’s the exercise. My uncle started doing tai chi and water aerobics three times a week after diagnosis. His tremors didn’t disappear, but his spirit did. Movement isn’t therapy - it’s rebellion.
Kelly Gerrard
The claim that dopamine replacement doesn't cure Parkinson's is scientifically accurate but emotionally misleading. Patients need hope not just facts. The fact that 70% experience dramatic improvement should be the headline not the footnote
Kunal Karakoti
It’s strange how we treat the brain like a machine that runs on fuel. But what if dopamine isn’t the problem? What if it’s the signal that’s corrupted? Maybe we’re pouring gasoline on a fire we don’t understand.
Cheyenne Sims
The article contains multiple grammatical inconsistencies and lacks peer-reviewed citations for key claims. While the intent is commendable, the presentation undermines its credibility. For instance, the phrase 'your body feels heavier than it should' is a subjective metaphor lacking clinical precision. Proper medical communication requires rigor, not anecdotal phrasing.