Liver Transplant Eligibility Calculator
Calculate Your MELD Score
The Model for End-Stage Liver Disease (MELD) score helps determine transplant urgency for patients with advanced liver disease. For genotype 3 hepatitis C, a score above 15 indicates significant risk and potential need for transplant.
When a patient with chronic hepatitis C genotype3 reaches end‑stage liver disease, a liver transplant surgical replacement of a diseased liver with a healthy donor organ can be a life‑saving option.
Key Takeaways
- Genotype3 progresses faster to cirrhosis and liver cancer than other HCV genotypes.
- Standard antiviral regimens often achieve lower cure rates for genotype3, especially in advanced disease.
- When MELD scores exceed 15 or decompensation occurs, transplantation offers the best chance of long‑term survival.
- Post‑transplant antiviral therapy dramatically reduces reinfection risk and improves graft longevity.
- Early referral to a transplant center cuts waiting‑list mortality by up to 30%.
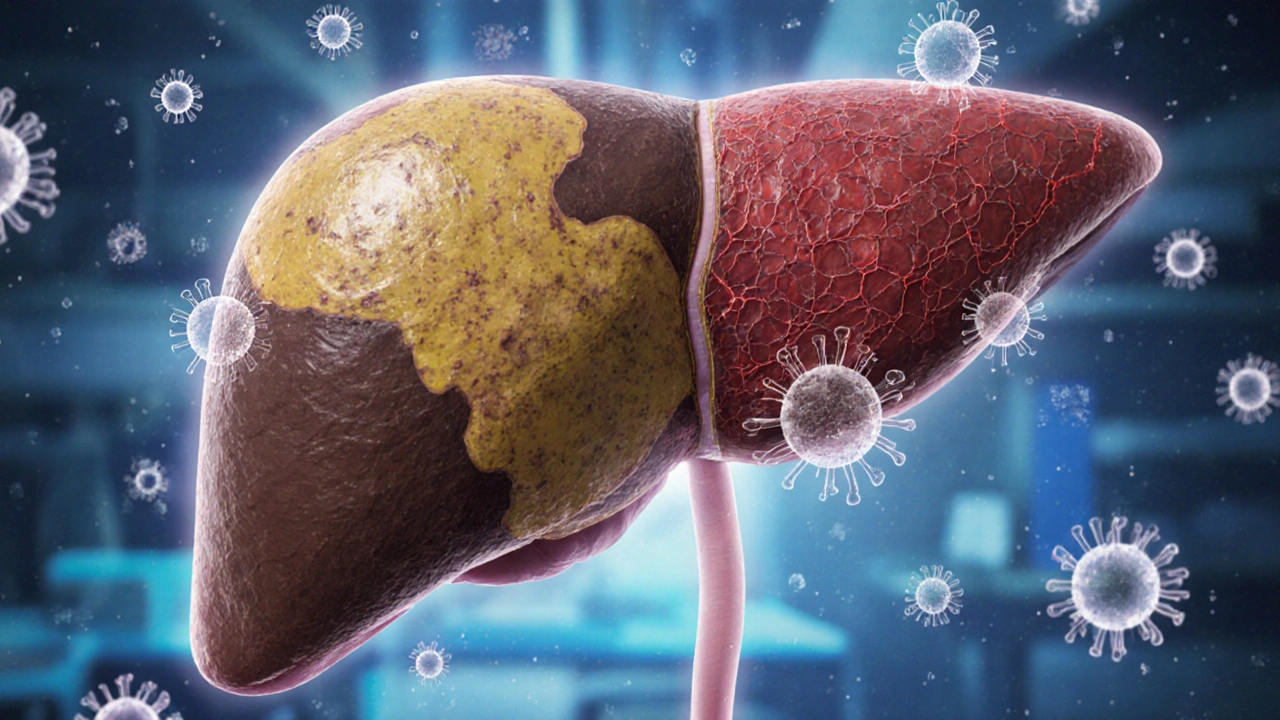
Understanding Genotype3 Hepatitis C
The genotype3 hepatitis C is a strain of the hepatitis C virus (HCV) that accounts for roughly 25% of global infections. It is notorious for causing rapid fat accumulation in liver cells, leading to steatosis, and for accelerating the transition from chronic inflammation to cirrhosis scarring of the liver that impairs its function. Studies from 2023‑2024 show a 1.5‑fold higher incidence of hepatocellular carcinoma in genotype3 patients compared with genotype1.
Because the virus mutates quickly, standard direct‑acting antivirals (DAAs) target specific proteins in the hepatitis C virus to stop replication achieve cure rates around 80‑85% in genotype3, versus 95% in easier‑to‑treat genotypes. The gap widens when the liver is already damaged.

When Transplant Becomes Necessary
Transplant candidacy hinges on objective measures of liver failure. The most widely used tool is the MELD score Model for End‑Stage Liver Disease, a numeric score predicting 90‑day mortality. A MELD score above 15 generally triggers referral, but genotype3 patients often decompensate at lower scores because of aggressive disease progression.
Key clinical signs include:
- Ascites (fluid buildup in the abdomen)
- Variceal bleeding from portal hypertension
- Encephalopathy (confusion due to toxin buildup)
- Jaundice persisting despite antiviral therapy
Early evaluation by a transplant multidisciplinary team can secure a spot on the waiting list before complications become irreversible.
Survival Benefits of Liver Transplant
Data from the United Kingdom Liver Transplant Registry (2024) reveal a 5‑year survival of 78% for genotype3 patients who receive a transplant, compared with 45% for those managed medically after decompensation. The survival advantage stems from two factors:
- Removal of the fibrotic organ eliminates the primary source of portal hypertension and toxin production.
- Post‑operative antiviral regimens achieve sustained virologic response (SVR) rates above 95% when combined with current DAAs.
Moreover, quality‑of‑life scores, measured by the Chronic Liver Disease Questionnaire, improve by an average of 30 points within six months post‑surgery.
Why Antiviral Therapy Alone May Not Suffice
DAAs remain the first‑line treatment for most HCV infections, but genotype3 poses distinct challenges:
| Approach | SVR Rate | Applicability in Cirrhosis | Typical Time to Success |
|---|---|---|---|
| DAA‑only (e.g., sofosbuvir/velpatasvir) | 80‑85% | Limited in Child‑Pugh B/C | 12 weeks |
| Liver transplant + post‑transplant DAA | 95‑98% | Applicable to all stages | 8‑12 weeks after surgery |
The lower SVR in cirrhotic patients translates into higher rates of HCV recurrence, graft failure, and mortality. Transplant therefore fills the therapeutic gap when the liver can no longer sustain life despite viral suppression.
Post‑Transplant Management
Successful graft survival hinges on three pillars:
- Immunosuppression medications that prevent the body from rejecting the donor liver - usually a calcineurin inhibitor combined with low‑dose steroids.
- Antiviral prophylaxis administration of DAAs soon after transplant to eradicate residual HCV - often a 12‑week course of glecaprevir/pibrentasvir.
- Regular monitoring of liver function tests and viral load, typically every month for the first year.
Reinfection rates have fallen from 30% in the pre‑DAA era to less than 5% after adopting routine post‑transplant antiviral therapy.
Practical Checklist for Patients and Clinicians
- Confirm HCV genotype using a reliable PCR assay - ensure it reports *genotype3*.
- Assess liver disease severity: calculate MELD score, evaluate for ascites, encephalopathy, and variceal bleeding.
- Refer to a transplant center when MELD >15 or when decompensation signs appear, even if SVR is achieved.
- Discuss donor options - deceased donor organs remain the backbone, but consider living‑donor transplantation if a suitable relative is available.
- Plan post‑operative antiviral regimen; coordinate with hepatology and transplant pharmacy teams.
- Schedule lifelong follow‑up: imaging for hepatocellular carcinoma surveillance, routine labs, and quality‑of‑life assessments.
Following this checklist can reduce waiting‑list dropout and improve post‑transplant outcomes.
Frequently Asked Questions
Can a genotype3 patient avoid transplant by using newer antivirals?
New DAAs have raised cure rates, but for patients who already have decompensated cirrhosis the liver cannot recover fully. In those cases, transplant remains the only curative option.
How long is the waiting period for a donor liver in the UK?
On average, patients with a MELD score above 15 wait 3-6 months. Those with higher urgency may receive an organ within weeks.
What are the most common complications after transplant?
Early complications include infection, biliary leaks, and acute rejection. Long‑term issues involve chronic rejection, metabolic syndrome, and rare recurrence of HCV if antiviral therapy is omitted.
Is living‑donor liver transplantation safe for the donor?
When performed in experienced centers, donor complications are low (<2%). Donors retain sufficient liver volume to function normally after regeneration.
Will insurance cover the cost of transplant and post‑operative antivirals?
In the UK, the NHS funds both the transplant surgery and the standard 12‑week DAA course for eligible patients. Private insurers typically follow similar policies.
For anyone battling genotype3 hepatitis C, the message is clear: early assessment, timely referral, and a combined surgical‑pharmacologic approach offer the best chance at a healthy future. liver transplant isn’t just an option; it’s often the decisive step that turns a grim prognosis into a survivable reality.

Elijah Mbachu
Remember, early evaluation by a hepatology team can shave months off the waiting list, so keep an eye on any uptick in fatigue or jaundice and let your doc know ASAP.
Sunil Rawat
Hey, I totally get how scary the numbers look, but the MELD calculator is just a tool – talk to a specialist and they'll walk you through every step.
David Ross
Honestly, the transplant process isn’t just about a score, it’s also about timing, support systems, and the right center, so stay hopeful, stay proactive, and keep your health team in the loop.
Henry Seaton
Look, if you live in the US you should be proud of our medical system, but you also need to push for a spot before your liver fails.
Baby Thingie
The guidelines clearly state that a MELD >15 warrants transplant referral; ensure your labs are up‑to‑date and schedule the evaluation promptly. :)
Abby Elizabeth
This whole thing feels like a drama series.
Amy Hamilton
Consider the broader picture: a liver transplant can be a second chance at life, an opportunity to reclaim dreams, and a reminder that our bodies are resilient when we give them a fighting chance.
Jordan Schwartz
Adding to that, cirrhosis can be managed with antiviral therapy for genotype 3, but once decompensation sets in, transplant becomes the definitive solution; stay on top of your meds and attend every follow‑up.
Nitin Chauhan
Don’t let fear hold you back-getting listed early means you’re ahead of the curve and gives you more control over your timeline.
ayan majumdar
yeah, just keep the docs updated and follow the transplant center’s checklist.
Johnpaul Chukwuebuka
In many African clinics, early referral to a transplant center has saved countless lives; share this info with anyone you know who’s struggling.
Xavier Hernandez
It’s a moral imperative that we allocate organs wisely, yet we must also ensure equitable access for all patients, regardless of background.
Angel Gallegos
Honestly, the whole transplant hype is overrated; most patients end up with complications and a lifetime of immunosuppression.
ANTHONY COOK
What you’re missing is that only the strong‑est nations get the best organs, and it’s high time we prioritize our own citizens over outsiders. 😂
Sunthar Sinnathamby
From a global health angle, the scarcity of donor livers is a shared crisis; collaboration between countries could boost availability, but politics often get in the way.
Tim Moore
It is incumbent upon the medical community to uphold the highest standards of fairness, ensuring that allocation policies are transparent, evidence‑based, and devoid of any nationalist bias.
Alfred Benton
Don’t be fooled by mainstream narratives; the transplant industry is heavily influenced by pharmaceutical lobbying, and the true risks are deliberately downplayed.
Helen Crowe
When we talk about genotype 3 hepatitis C, the viral kinetics are notoriously aggressive, often leading to a rapid progression of fibrosis and steatosis, which in turn accelerates the rise of the MELD score.
Clinically, patients present with elevated AST/ALT ratios, persistent hyperbilirubinemia, and coagulopathy, all of which feed into the MELD calculation.
Research shows that a MELD >15 in this subgroup correlates with a 30% increase in 1‑year mortality if transplantation is delayed.
Therefore, early referral to a transplant center is not merely advisable; it is a critical intervention to curb the cascade of decompensation.
Moreover, antiviral therapy with sofosbuvir‑velpatasvir can achieve SVR rates above 95%, but in patients with advanced cirrhosis the therapeutic window narrows considerably.
Hence, a combined approach-optimizing antiviral regimens while simultaneously evaluating transplant candidacy-maximizes survival odds.
From a logistical standpoint, the United Network for Organ Sharing (UNOS) prioritizes MELD scores but also considers exception points for rapid disease progression, which genotype 3 patients frequently qualify for.
In practice, assembling a multidisciplinary team-including hepatology, transplant surgery, nutrition, and psychosocial support-ensures that candidates meet both medical and psychosocial criteria.
Nutrition plays a pivotal role; sarcopenia is a known predictor of poor post‑transplant outcomes, so early dietary intervention can improve transplant eligibility.
Psychosocial evaluation, often overlooked, assesses adherence potential and support networks, both of which are vital for post‑operative success.
Donor-recipient matching also hinges on blood type compatibility and size matching, but for genotype 3 patients the urgency often outweighs minor HLA mismatches.
Immunosuppression protocols have evolved, with tacrolimus‑based regimens now standard, yet patients must be educated about infection risks and metabolic side effects.
Long‑term follow‑up includes regular imaging to monitor for hepatocellular carcinoma, a known complication in chronic hepatitis C cirrhosis.
In summary, a MELD score exceeding 15 in genotype 3 hepatitis C patients is a red flag that should trigger immediate multidisciplinary evaluation, antiviral optimization, and transplant listing to improve both short‑ and long‑term outcomes.