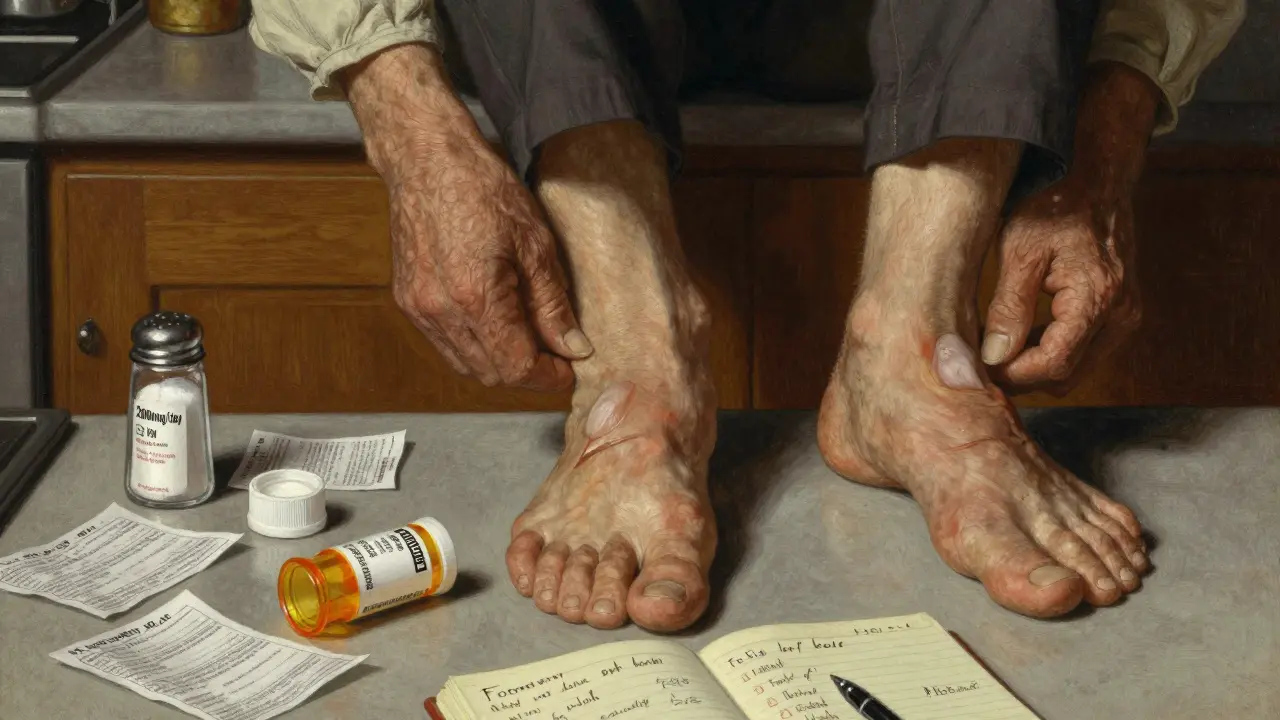
When your kidneys start to fail, fluid doesn’t just disappear-it builds up. Swollen ankles, puffy eyes, a bloated belly-these aren’t just inconveniences. They’re warning signs. In chronic kidney disease (CKD), edema happens because the kidneys can’t flush out sodium and water like they used to. The result? Too much fluid pooling in your tissues. And if left unchecked, it can lead to high blood pressure, heart strain, and even hospitalization.
Why Edema Happens in CKD
Your kidneys are your body’s main fluid regulators. When they’re healthy, they filter out extra sodium and water every day. But as CKD progresses-especially in stages 3 to 5-this system breaks down. Sodium sticks around, pulling water with it. Blood volume increases. Pressure builds in your capillaries. Fluid leaks into your skin, legs, and sometimes your belly. This isn’t just about drinking too much water. It’s about your body’s inability to excrete sodium. Even if you drink less, if your kidneys can’t remove sodium, fluid keeps accumulating. That’s why simply cutting back on fluids alone rarely fixes the problem. You have to tackle sodium first.Diuretics: The Medication Tool
Diuretics are the go-to drugs for flushing out excess fluid. But not all diuretics work the same way, especially in CKD. For people with eGFR below 30, loop diuretics like furosemide, bumetanide, or torsemide are the standard. They work on the loop of Henle in the kidney, a spot that’s still active even when other parts are damaged. A typical starting dose is 40-80 mg of furosemide daily. If that doesn’t help, doctors may increase it by 20-40 mg every few days-up to 320 mg in severe cases. But here’s the catch: diuretics don’t come without risk. A 2016 NIH study found that CKD patients on diuretics lost kidney function 3.2 mL/min/1.73m² per year, compared to 1.7 mL/min/1.73m² in those not taking them. That’s nearly double the decline. And if you take too much-especially above 160 mg of furosemide daily-you raise your risk of sudden kidney injury by over four times. That’s why doctors are shifting toward slower, steadier fluid removal. The goal isn’t to drain you dry overnight. It’s to reach your “dry weight”-the lightest weight you can safely maintain without swelling or dizziness. For patients with eGFR above 30, thiazide diuretics like hydrochlorothiazide can help. But when loop and thiazide are combined-called sequential nephron blockade-the effect is stronger. The downside? A 23% higher chance of acute kidney injury. So this combo is reserved for stubborn cases. Spironolactone is another option, especially if you also have heart failure. It helps reduce fluid and even cuts mortality risk by 30% in severe heart failure with CKD. But it’s risky if your potassium is already high. In stage 4 or 5 CKD, over 25% of patients on spironolactone develop dangerous hyperkalemia. Regular blood tests are non-negotiable.Salt Restriction: The Foundation
Medication alone won’t fix edema if you keep eating like you did before CKD. The National Kidney Foundation recommends no more than 2,000 mg of sodium per day for anyone with CKD and swelling. For advanced stages (4 and 5), they suggest dropping to 1,500 mg. That’s less than one teaspoon of salt. But here’s the problem: most sodium isn’t from the salt shaker. It’s hidden. Two slices of bread? 300-400 mg. One cup of canned soup? 800-1,200 mg. Two ounces of deli meat? 500-700 mg. Even yogurt and fruit can add up-yogurt has about 200 mL of fluid per cup, and watermelon is 92% water. Strict sodium restriction can reduce swelling by 30-40% in early CKD-without any pills. But it’s hard. People report taste loss, social isolation, and frustration. A 2024 survey found 68% of CKD patients struggle to stick to low-sodium diets. That’s why working with a renal dietitian matters. Three to four sessions can teach you how to read labels, swap out processed foods, and cook flavorful meals with herbs instead of salt. Fluid intake matters too. In advanced CKD, doctors often cap total fluid at 1,500-2,000 mL per day. That includes soups, ice, sauces, and even fruits. Tracking everything you drink and eat is the only way to stay in control.
Compression Therapy: The Physical Support
When swelling lingers in your legs, compression isn’t optional-it’s essential. Graduated compression stockings (30-40 mmHg at the ankle) are the gold standard. They squeeze your legs tighter at the bottom and looser at the top, pushing fluid back toward your heart. Studies show they can reduce leg volume by 15-20% in just four weeks. But most people stop wearing them. A 2022 study found only 38% kept using them after three months. Why? They’re hard to put on, cause skin irritation, and feel uncomfortable. That’s why pairing them with movement helps. Walking 30 minutes five days a week improves lymphatic drainage and cuts swelling by 22% compared to sitting still. For severe cases-especially with nephrotic syndrome-intermittent pneumatic compression devices offer more. These machines inflate and deflate around your leg in cycles, mimicking muscle movement. One 2020 study found they reduced leg circumference 35% more than regular stockings. Elevating your legs above heart level for 20-30 minutes a few times a day also helps. It’s simple, free, and effective. Just don’t do it while sitting with your legs dangling-that doesn’t count.Putting It All Together
There’s no single fix for edema in CKD. It’s a three-part system:- Salt restriction reduces the root cause: sodium overload.
- Diuretics help your kidneys flush what they can’t remove on their own.
- Compression and movement manage the visible swelling and prevent complications like skin breakdown or blood clots.
The Real Risks and Trade-Offs
Doctors walk a tightrope. Too little fluid removal? Risk of heart failure, pulmonary edema, death. Too much? Risk of low blood pressure, kidney damage, or needing dialysis sooner. Dr. David Wheeler, a lead author of the KDIGO guidelines, says: “The window for diuretics in advanced CKD is narrow.” He’s not against them-he’s against reckless use. Meanwhile, Dr. Ronald J. Falk of the American Society of Nephrology reminds us: “Untreated volume overload carries greater mortality risk than judicious diuretic use.” The data backs him up. People with persistent edema have a 28% higher risk of dying than those who achieve dry weight. That’s why treatment isn’t one-size-fits-all. A 65-year-old with stage 3 CKD and mild swelling might do fine with salt restriction and walking. A 72-year-old with stage 5 CKD, heart failure, and 10-pound leg swelling? They need the full package: low-sodium diet, diuretic titration, compression, and frequent monitoring.What’s Next?
New tools are on the horizon. The NIH’s FOCUS trial, ending in late 2025, is testing whether using bioimpedance spectroscopy (BIS)-a device that measures body fluid levels-can make diuretic dosing more precise. Early results show a 32% drop in hospital visits for fluid overload. The FDA’s March 2025 approval of IV furosemide for advanced CKD is another big step. For patients with eGFR under 15, IV delivery clears fluid 38% better than pills. That’s huge for those who can’t absorb oral meds. Vaptans, drugs that block water retention hormones, showed promise but were paused due to liver risks. So for now, the triad of salt, diuretics, and compression remains the backbone of care.What You Can Do Today
If you’re living with CKD and swelling:- Track your sodium. Use an app or journal. Aim for under 2,000 mg daily.
- Read every food label. Avoid anything with more than 200 mg sodium per serving.
- Ask your doctor if you need a diuretic-and if so, which one. Don’t self-adjust doses.
- Try compression stockings. Start with 20-30 mmHg if 30-40 is too tight.
- Walk daily. Even 15 minutes helps.
- See a renal dietitian. It’s not a luxury-it’s part of your treatment plan.
Can I stop taking diuretics if I eat less salt?
Sometimes, yes-but only under medical supervision. In early-stage CKD, strict salt restriction can reduce swelling enough to lower or eliminate diuretic needs. But in advanced stages, your kidneys may still need help flushing fluid. Stopping diuretics without a plan can cause rapid fluid buildup. Never stop or change your dose without talking to your nephrologist.
Why do I still swell even though I’m on diuretics?
Diuretics work best when sodium intake is low. If you’re still eating high-sodium foods, your body holds onto water faster than the pills can remove it. Also, in late-stage CKD, your kidneys become less responsive to diuretics. You might need a higher dose, a different type, or combination therapy. Compression and movement also help where pills alone fall short.
Are compression stockings really necessary if I’m not active?
Yes-even if you’re not walking much, compression helps. When you sit or lie down, gravity pulls fluid into your legs. Compression stockings counteract that by pushing fluid upward. Without them, swelling worsens, skin becomes fragile, and risk of ulcers or infection rises. Movement helps, but compression provides constant support.
Can drinking more water help flush out sodium?
No. In CKD, your kidneys can’t process extra water efficiently. Drinking more doesn’t flush out sodium-it just adds to the fluid overload. That’s why fluid limits are part of the treatment. Your goal isn’t to drink more to cleanse; it’s to drink less to avoid swelling.
How long does it take to see results from salt restriction?
Most people notice less swelling in 2-4 weeks with consistent sodium control. Weight loss of 1-2 pounds per week is typical. The key is consistency. One high-sodium meal can undo days of progress. Keep tracking, keep cooking low-sodium meals, and your body will respond.
Is it safe to use over-the-counter diuretics for CKD swelling?
No. Over-the-counter diuretics (like herbal supplements or caffeine pills) are not safe for CKD. They can cause dangerous electrolyte imbalances, worsen kidney function, or interact with your prescription meds. Only use diuretics prescribed and monitored by your kidney doctor.



Eli Kiseop
So basically if I stop eating salt my legs won't swell anymore? That sounds too good to be true
Been trying to cut back but my pizza and chips are fighting me
Dan Pearson
LMAO you people think this is rocket science? In America we fix this with salt, diuretics, and a damn good steak. If your kidneys can't handle it maybe you shouldn't have eaten that Taco Bell in the first place. #AmericanMedicine #FixItOrQuitIt
Ellie Norris
Just a quick note-compression stockings can be a pain to put on but i found these silicone grip ones on amazon that make it way easier. Also, dont forget to moisturize your legs daily, dry skin + compression = bad news.
ps: typo sorry lol
Marc Durocher
Y'all are making this way harder than it needs to be. I've got a buddy with stage 4 CKD who eats tacos every Friday, drinks soda, and still walks 2 miles a day with his compression socks on. He's got less swelling than half the people in this thread. Sometimes it's not about perfection-it's about consistency.
Also, if you're not walking, you're basically just storing fluid like a water balloon. Move your legs, folks.
larry keenan
The physiological mechanism underlying fluid retention in chronic kidney disease involves dysregulation of the renin-angiotensin-aldosterone system, coupled with impaired natriuresis. Diuretic efficacy is contingent upon glomerular filtration rate thresholds, with loop diuretics demonstrating preferential activity at the thick ascending limb of the loop of Henle. Compression therapy exerts mechanical pressure gradients that enhance venous return and lymphatic drainage, thereby mitigating dependent edema. These interventions constitute a tripartite therapeutic paradigm supported by KDIGO 2023 clinical guidelines.
Nick Flake
Man… I just wanna say this hit me right in the soul 🥹
It’s not just about medicine. It’s about dignity. When your legs swell so much you can’t fit into your favorite shoes? That’s not a symptom-it’s a loss.
But here’s the beautiful part: you can take it back. Salt check. Socks on. Walk outside. One step. One meal. One day.
You’re not broken. You’re adapting. And that’s brave.
❤️🫶
Akhona Myeki
As a South African nephrologist, I must emphasize that the Western approach to CKD is fundamentally flawed. You over-medicalize everything. In our rural clinics, we use traditional herbs, salt restriction, and elevation. No pills. No expensive stockings. Just community, discipline, and respect for the body's rhythm. Your pharmaceutical industry profits from your dependency. Question the system.
Chinmoy Kumar
Hey just wanted to say this post helped me a lot. I was scared to even talk to my doc about diuretics but now i feel like i know what to ask. Also i started tracking my sodium with an app and wow… i had no idea how much was in bread. Thanks for the real talk. Keep it up!
Brett MacDonald
So if I stop eating salt and take diuretics and wear socks… am I basically becoming a human filter?
Feels like I’m turning into a sci-fi character. "Subject 7: Sodium-Neutralized Human. Output: Slightly Less Swollen."
Also, why do I feel like I’m being punished for existing?
Sandeep Kumar
Why are we even talking about this? In India we just drink neem water and walk barefoot on grass. No fancy meds. No compression gear. Your western medicine is just a money trap. Real healing is simple. You just need willpower. And maybe stop eating cheese.
Gary Mitts
My mom’s been on this regimen for 3 years. She lost 12 pounds of fluid. No hospital visits. Still eats ice cream once a week.
It works if you stick with it.
That’s it.
Ansley Mayson
So let me get this straight. You’re telling me I have to give up my Doritos, my soup, my deli meat, my yogurt, my watermelon, and my daily nap because my kidneys are lazy?
And now I have to wear socks that feel like a vise?
And walk?
And pay a dietitian?
And get blood tests?
And hope the diuretics don’t kill my kidneys faster?
...I’ll just die then.