
When melanoma is caught early, the chance of surviving five years is over 99%. But if it spreads, that drops to just 32.1%. This stark difference is why catching melanoma early can be life-saving. Melanoma is a type of skin cancer that starts in melanocytes-the cells that give skin its color. Unlike other skin cancers, it grows fast and spreads easily, making early detection critical.
Why Early Detection Changes Everything
Most people know melanoma as "skin cancer," but it’s the deadliest type. The American Cancer Society’s 2025 data shows localized melanoma has a 99%+ survival rate, but once it spreads to distant organs, survival plummets to 32.1%. This isn’t just a statistic-it means catching it before it moves saves lives. Think of it like a wildfire: smother it early, and it’s manageable. Let it spread, and it becomes a disaster.
Traditional Detection: What Works and What Doesn’t
For decades, doctors checked moles with the naked eye or a dermatoscope (a magnifying tool). Dermoscopy is still used today, but it’s not perfect. Primary care doctors spot only 60-70% of melanomas during routine exams. Even dermatologists miss cases-especially in hard-to-see spots like under nails or on the scalp.
Here’s the problem: melanoma often looks like a harmless mole. A mole with uneven color or an irregular border? That’s a red flag. But many people ignore changes until it’s too late. Skin Cancer isn’t just about sunburns-it’s about recognizing subtle shifts in your skin. The ABCDE rule helps: Asymmetry, irregular Borders, Color variation, Diameter larger than 6mm, and Evolving changes.
How AI and Wearables Are Revolutionizing Detection
New tech is filling the gaps. AI Detection systems like SegFusion from Northeastern University combine image segmentation and classification. They analyze dermoscopic photos with 95% sensitivity and 87% specificity-outperforming human eyes.
Let’s break it down. SegFusion first isolates suspicious skin areas (segmentation), then classifies them (classification). This two-step process handles real-world challenges like uneven lighting or dark skin tones. In trials, it flagged melanomas doctors missed. But AI isn’t perfect. SegFusion still needs clinical validation before widespread use.
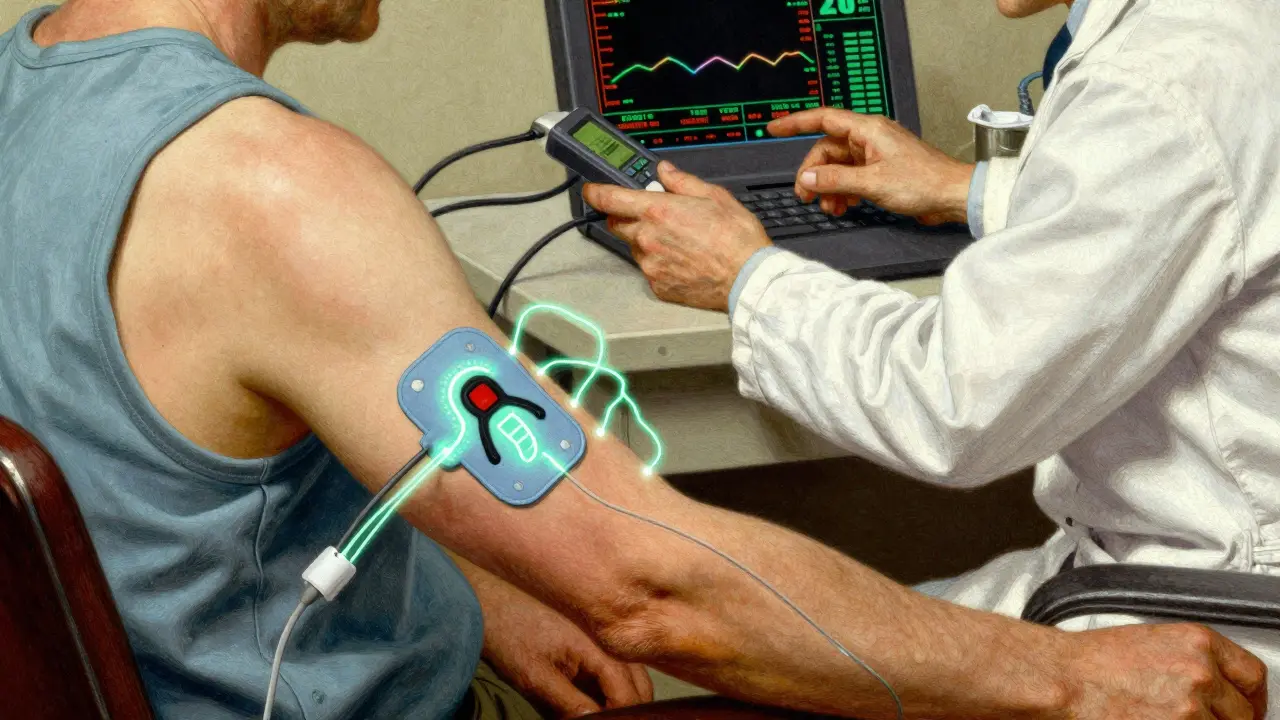
Another breakthrough: wearable patches. Bioimpedance sensors from Wake Forest University measure electrical differences between healthy and cancerous tissue. The battery-free patch connects to a small reader device and detects abnormalities in seconds. Early tests on 10 volunteers showed statistically significant differences (p<0.05), but larger studies are needed. Patients describe it as "comfortable for extended wear," though electrode design needs tweaks.
Then there’s the EU’s iToBoS project. This full-body scanner maps every mole in six minutes. It uses explainable AI (XAI) to show doctors why a spot is flagged-critical for trust. In European clinics, dermatologists report 78% satisfaction but want to reduce false positives (currently 35%).
How Immunotherapy Is Transforming Treatment
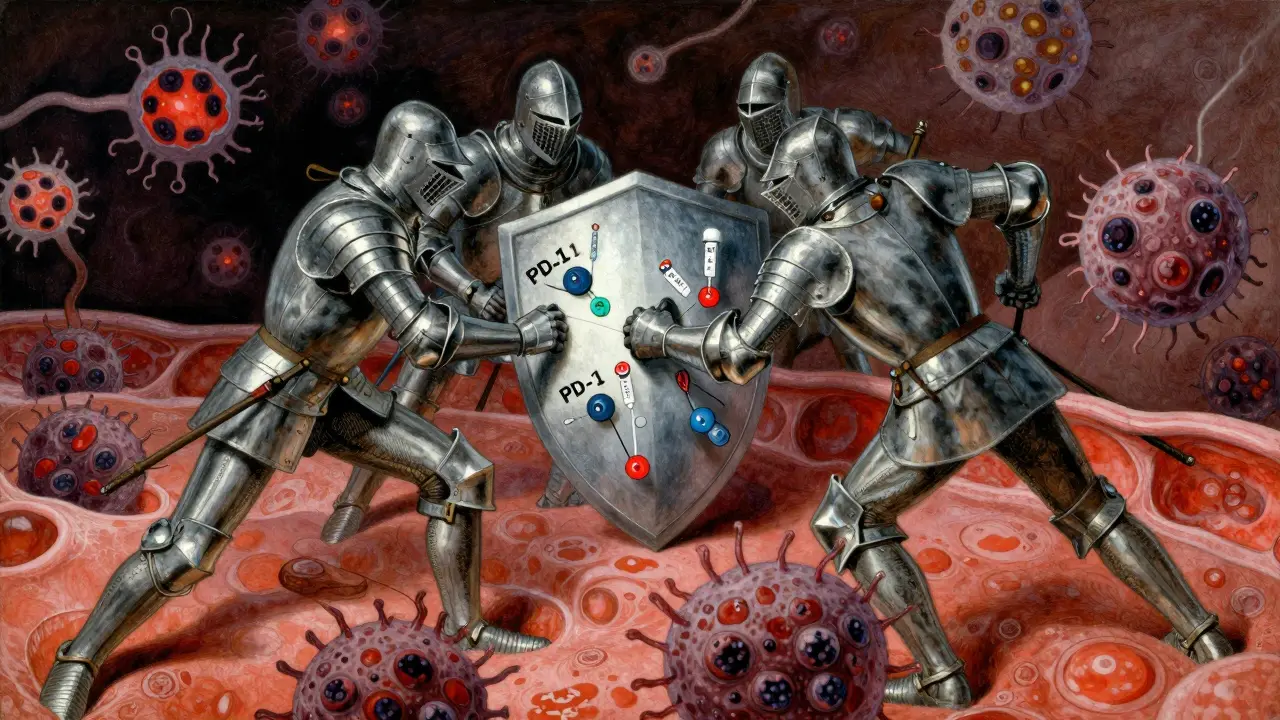
For advanced melanoma, immunotherapy is a game-changer. Immunotherapy works by boosting your immune system to attack cancer cells. Unlike chemotherapy, it targets only cancerous tissue, reducing side effects.
How? Drugs like PD-1 inhibitors (e.g., pembrolizumab) and CTLA-4 inhibitors (e.g., ipilimumab) block signals that hide cancer from immune cells. When used together, they double response rates compared to single-drug therapy. Since the FDA approved ipilimumab in 2011, survival rates for metastatic melanoma have jumped from 10% to over 50% in long-term studies.
But it’s not magic. Some patients don’t respond. Others face immune-related side effects like rashes or fatigue. New trials are testing combinations. Regeneron’s fianlimab (a LAG-3 blocker) with a PD-1 drug is showing promise in Phase 3 trials. Meanwhile, the SUPRAME trial is evaluating IMA203 PRAME cell therapy-a personalized treatment for patients with specific genetic markers.
What You Should Know Right Now
Here’s how to stay ahead:
- Check your skin monthly. Use a mirror for hard-to-see spots.
- Know your ABCDEs. If a mole changes size, color, or shape, see a dermatologist.
- Ask about new tools. Dermatologists increasingly use AI-assisted tools like DermaSensor (FDA-approved in 2024) for extra confidence.
- Don’t skip annual skin checks if you have risk factors: fair skin, family history, or lots of sun exposure.
DermaSensor is a handheld device that measures light scattering. Primary care doctors say it boosts confidence-87% felt more sure after training. But it has low specificity (26-40%), meaning it often flags harmless moles. That’s why it’s a supplement, not a replacement, for expert evaluation.
The Future of Melanoma Care
Researchers are combining imaging, genetics, and AI for personalized care. Immunotherapy is evolving too. New drugs target specific mutations, and cell therapies like IMA203 PRAME are showing 56% complete response rates in early trials.
But challenges remain. AI tools struggle with diverse skin tones-JAMA Dermatology found they’re 12-15% less accurate on darker skin. Regulatory hurdles slow adoption; FDA clearance takes 18-24 months. Still, the market is growing fast. By 2030, AI-assisted detection could become standard care, potentially cutting melanoma deaths by 40-50%.
Comparison of Melanoma Detection Methods
| Method | Sensitivity | Specificity | Key Features |
|---|---|---|---|
| Visual Inspection (Primary Care) | 60-70% | 65-75% | Low cost, widely available |
| Dermoscopy (Dermatologist) | 85-90% | 75-85% | Requires specialized training |
| DermaSensor (ESS) | 85-95% | 26-40% | FDA-approved for non-dermatologists |
| SegFusion AI | 95% | 87% | Combines segmentation and classification |
Can AI replace dermatologists for melanoma detection?
No, AI is a tool to assist doctors, not replace them. Current systems like SegFusion and DermaSensor help identify suspicious lesions but still require clinical evaluation. Dermatologists use AI results alongside their expertise to make final decisions. As Dr. Neha Chaudhary from Northeastern University explains, "AI will clearly tell you whether a lesion is cancerous, but human judgment is still essential for treatment decisions."
What’s the biggest risk of new detection tech?
Overdiagnosis. Tools like DermaSensor have low specificity (26-40%), meaning they often flag benign moles as cancerous. This leads to unnecessary biopsies, anxiety, and costs. Experts like the Taylor & Francis team warn that "screening can detect melanoma earlier but may cause excess morbidity with little survival benefit" if not paired with careful clinical follow-up.
Is immunotherapy effective for all melanoma patients?
Not yet. About 40-50% of patients respond to current immunotherapies. New approaches like personalized cell therapies (e.g., IMA203 PRAME) and combination drugs (e.g., fianlimab + PD-1 inhibitors) aim to help more people. Trials show promising results-56% complete response in early studies-but these treatments aren’t widely available yet.
How can I access these new treatments?
For detection, ask your dermatologist about AI tools like DermaSensor (FDA-approved for primary care use). For advanced melanoma, immunotherapy is standard care at major cancer centers. Clinical trials for newer therapies (like SUPRAME) are open at hospitals like Mayo Clinic and Cleveland Clinic. Your doctor can help determine eligibility.
What’s the best way to prevent melanoma?
Sun protection is key. Wear UPF 50+ clothing, use broad-spectrum sunscreen daily, and avoid tanning beds. But prevention isn’t enough-early detection saves lives. Check your skin monthly and see a dermatologist yearly, especially if you have risk factors like fair skin or a family history.





Georgeana Chantie
This is why America needs to lead in melanoma research! We're better than Europe and Asia at this. 😤
Jennifer Aronson
The data presented here is compelling. However, access to dermatologists varies globally. Cultural factors influence early detection rates.
Kate Gile
Early detection saves lives! Let's spread awareness and get regular skin checks.
Gregory Rodriguez
Wow, AI's better than docs at spotting melanoma? Next they'll replace all doctors with a smartphone app. 😏
anjar maike
AI tech is great but rural areas lack access to healthcare. 🤔
Arjun Paul
This tech is useless without proper healthcare infrastructure. We need to fix basics first.
divya shetty
It's irresponsible to promote AI without addressing data bias. Many models fail on darker skin tones.
Nancy Maneely
This is why America's healthcare is failin'! They're too busy with AI to fix real problems. 😭
Phoebe Norman
The bioimpedance sensors are interesting but lack clinical validation. The p-value is not significant enough for real-world use.
Albert Lua
This is important globally! In my travels across India and Africa, I've seen firsthand how melanoma affects different populations. The lack of awareness in rural areas is staggering. Many people don't even know what melanoma is. They think it's just a mole, not a life-threatening cancer. Sun exposure is a big issue, especially in places with high UV index. But healthcare infrastructure is lacking. You can't have AI detection if people can't even see a doctor. The SegFusion system is cool, but it's useless without proper training for local doctors. Wearable patches are promising, but battery-free tech isn't widely available yet. We need to invest in education and infrastructure first. Otherwise, all this tech is just for the privileged. It's not just about the science; it's about equity. Melanoma doesn't care about borders or skin color. We need a global approach. Let's not forget prevention-sunscreen, hats, avoiding peak sun. This isn't just a US problem; it's a worldwide issue that needs collaboration.
Katharine Meiler
The current AI models show promising sensitivity but specificity needs improvement. More diverse datasets are required.
Lana Younis
Hey folks, melanoma's not just a 'white people' problem. Darker skin tones can get it too. Let's all check each other out. 😊
Matthew Morales
AI's cool but let's not forget regular checkups. My buddy had a mole removed last yar, all good. 👍
Dr. Sara Harowitz
This is why we need more US-led research! The current studies are too reliant on foreign data. It's unacceptable!!!