
The Red Flags: How to Spot the Signs
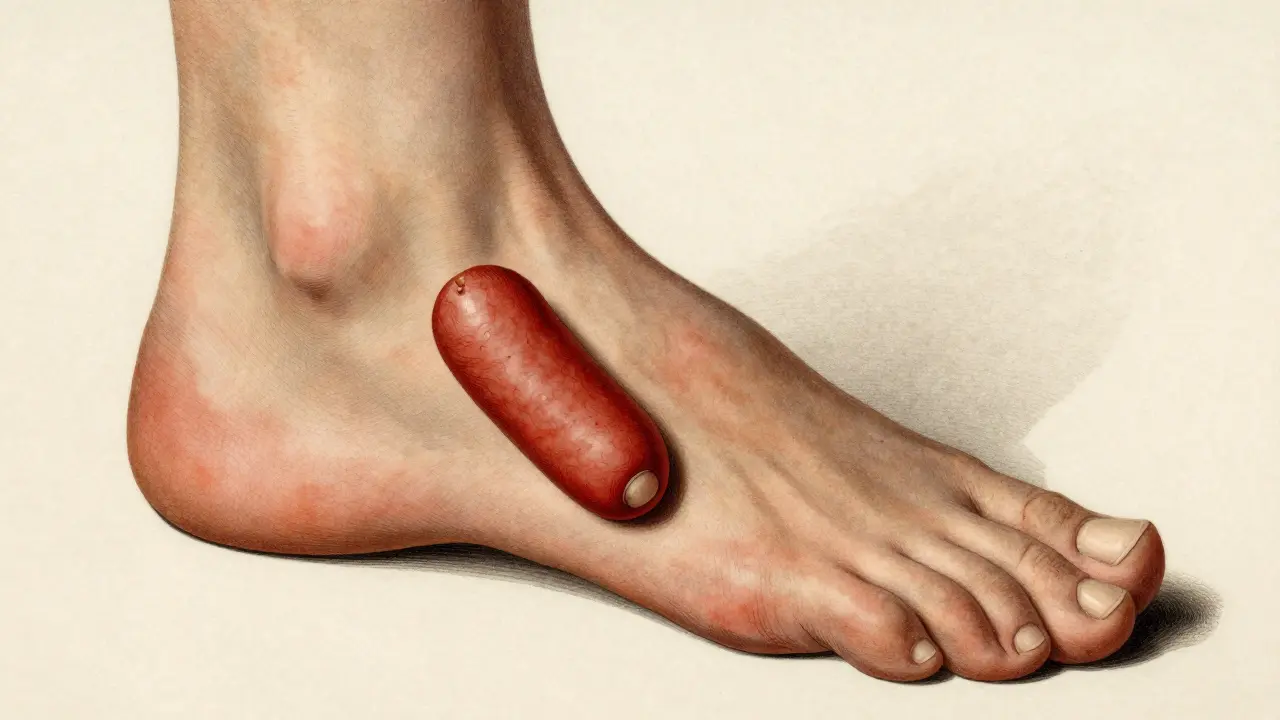
Identifying this condition isn't always straightforward because it doesn't hit everyone the same way. Unlike some forms of arthritis that mirror each other on both sides of the body, this often shows up asymmetrically. You might have a swollen right ankle but a perfectly fine left one. One of the most distinct signs is Dactylitis, which looks like "sausage digits." This happens when an entire finger or toe swells up, making it look plump and cylindrical. About 40-50% of patients experience this. Then there is Enthesitis, which is inflammation where tendons or ligaments attach to the bone. If you have chronic Achilles tendinitis or plantar fasciitis that won't go away, it might not be an injury-it could be your immune system attacking those attachment points. Your nails are also a huge clue. While standard skin psoriasis causes plaques, those with joint involvement often see pitting (tiny dents in the nail) or onycholysis, where the nail actually separates from the bed. In fact, 80-90% of people with this condition show nail changes, compared to only 10-50% of those with just skin psoriasis.The Five Ways it Manifests
Not all cases look the same. Depending on which part of your immune system is overreacting, you might fall into one of these five patterns:- Symmetric Polyarthritis: This affects multiple joints on both sides of the body, mimicking some other types of arthritis. It's seen in about 25% of cases.
- Asymmetric Oligoarthritis: This is the most common version (affecting 70% of patients), where only a few joints are involved, and they aren't mirrored on the opposite side.
- Distal Interphalangeal Predominant: This specifically targets the joints closest to your fingernails and toenails.
- Spondylitis: This causes inflammation in the spine and sacroiliac joints, leading to chronic back pain and stiffness.
- Arthritis Mutilans: A rare but severe form (less than 5%) that can lead to the total collapse of the joint structure.
Comparing the Big Players: Psoriatic vs. Rheumatoid Arthritis
It's very common for patients to be misdiagnosed with rheumatoid arthritis (RA) initially. However, the two are biologically different. RA is usually symmetric and often shows a positive "rheumatoid factor" in blood tests. Psoriatic arthritis, on the other hand, is usually asymmetric, involves the skin and nails, and is negative for rheumatoid factor in 90% of patients.| Feature | Psoriatic Arthritis | Rheumatoid Arthritis |
|---|---|---|
| Joint Pattern | Often Asymmetric | Usually Symmetric |
| Skin/Nail Involvement | Very Common (Plaques, Pitting) | Rare |
| Dactylitis (Sausage Digits) | Frequent (40-50%) | Very Rare |
| Blood Markers | Usually RF Negative | Often RF Positive (70-80%) |
Modern Treatment Paths
We've come a long way since the 1990s. The goal now is "treat-to-target," which means adjusting medication until you reach minimal disease activity. If you catch it early-ideally within 12 weeks of the first symptom-you can prevent irreversible joint damage in up to 75% of cases.Treatment usually starts with DMARDs (Disease-Modifying Antirheumatic Drugs). These are the foundation and help slow down the progression of the disease. But for many, the real game-changer is the use of biologics.
Biologics are engineered proteins that target specific parts of the immune system. For example, TNF inhibitors like adalimumab or etanercept are staples in treatment, making up over half of all biologic prescriptions. Newer options like TYK2 inhibitors (such as deucravacitinib) provide a more targeted approach, often coming in oral forms that avoid the needle entirely.

The Reality of Living With It
Medication is only half the battle. Many patients report a persistent "brain fog" and crushing fatigue that doesn't always disappear even when the joint swelling is gone. It's also a financial burden; many of these high-tech drugs come with steep out-of-pocket costs. Managing this requires a team. You can't just see a GP. You need a rheumatologist for the joints, a dermatologist for the skin, and often a physical therapist to keep your mobility from slipping. It usually takes about 3 to 6 months of tracking your own symptoms before you can identify your specific triggers-whether it's stress, certain foods, or weather changes.What's on the Horizon?
We are moving toward a world of personalized medicine. Researchers are currently using AI algorithms to predict who will develop joint issues by analyzing nail and joint imaging with 87% accuracy. By 2028, genetic markers may allow doctors to skip the "trial-and-error" phase and put you on the exact medication your body needs from day one. While the risk of cardiovascular disease is 1.5 times higher for those with this condition, the outlook is generally positive. With modern management, most people can expect a near-normal life expectancy. The key is not waiting for the joints to "stiffen up" before seeking help-early intervention is the only way to protect your mobility for the long haul.Can I have joint pain without having any skin rashes?
Yes. About 15% of people develop joint symptoms before any skin manifestations appear. This is why many cases are initially misdiagnosed as other types of arthritis.
What are the most common types of skin psoriasis associated with this?
Plaque psoriasis is the most frequent, affecting 80-90% of patients. Other types include guttate psoriasis (often following a strep infection), inverse psoriasis in skin folds, and the more severe pustular or erythrodermic versions.
Are there side effects to biologic treatments?
Yes, some patients experience injection site reactions. More importantly, because biologics modulate the immune system, you must be screened for tuberculosis and hepatitis before starting therapy to ensure the medication doesn't trigger a latent infection.
How does a doctor diagnose this if there is no specific blood test?
Diagnosis is based on clinical markers: the pattern of joint involvement (asymmetric), the presence of dactylitis, nail pitting, and a personal or family history of psoriasis. Imaging and the absence of rheumatoid factor also help narrow it down.
Will this condition eventually lead to permanent joint damage?
It can if left untreated. Research shows that 30% of patients develop significant joint damage within two years of onset if they aren't on the right medication. However, early treatment within 12 weeks can prevent irreversible damage in 75% of cases.




william wang
The bit about the "sausage digits" is a huge tell. I've seen so many people mistake dactylitis for just a bad sprain or a weird allergic reaction, but once you know what to look for, it's a game changer for getting to the right specialist faster. It's also worth mentioning that keeping a daily joint diary for those first few months really helps the rheumatologist map out the asymmetry since it's hard to remember exactly which knuckle was swollen three weeks ago.
Joshua Nicholson
Too long, but the tips are alright I guess.
Cheryl C
Omg my cousin had this and the meds here in USA are just the best in the world!! 🇺🇸✨🇺🇸 Some of these other countries prolly dont even have biologics yet lol! Just imagine having to deal with stiff joints without our amazing healthcare system 💅💊🇺🇸
Josephine Wyburn
I literally cannot even describe the absolute agony of waking up and feeling like my entire body is made of rusted metal and broken glass 😭💔 it's just so unfair that we have to deal with this crushing fatigue while everyone else is just walking around acting like everything is fine in their perfect little lives... the brain fog makes me feel like I'm disappearing into a void and nobody even notices the struggle 🌧️🥀🫠
Ben Ferguson
It is truly a fascinating exploration of the human condition that our own immune system, designed to be our most fierce protector and loyal sentinel, can suddenly turn its gaze inward with such devastating precision, transforming the very act of movement into a choreographed dance of pain and resilience, reminding us that the boundary between health and illness is often as thin as a single cell's mistaken identity in the grand tapestry of biological existence.
Randall Barker
People love to talk about the 'science' of biologics but they ignore the fundamental moral failure of a system that prices these drugs so high that only the elite can afford to walk without pain. We are treating human health as a luxury commodity, which is a philosophical bankruptcy of the highest order. If you can't access the medicine, the 'personalized AI' the post mentions is just a futuristic fairy tale to keep the poor hopeful while their joints collapse.
Heer Malhotra
The focus on Western pharmaceutical triumphs is quite tiresome. India has provided the world with an abundance of generic medications and holistic integration that far surpasses the greed-driven models of the West. It is a matter of national pride that our medical infrastructure is evolving to provide these services with a level of equity and moral standing that your expensive biologics will never achieve.
Adele Shaw
Exactly. The US system is a joke and it's basically an assault on the poor. I've spent years fighting for coverage and it's just a nightmare of paperwork and lies. Absolute garbage.